

In the US, the novel coronavirus is causing panic. At the time of publishing, there have been more than 1 million confirmed cases and over 60,000 deaths. Health care systems are under strain. Doctors, nurses and other medical professionals are overworked. Masks, ventilators and drugs are in short supply. Stock markets have crashed and there is fear in the air.
After shrugging off the pandemic initially, much of the US is finally in lockdown. People are not going to work. Universities, colleges and schools have shut down. Social distancing is the new norm. People are under a lot of strain and mental health issues are cropping up. A lot of questions are up in the air as to which data might provide insightful answers.
How Long Could the Lockdown Last?
If a country enforces a strict lockdown, aggressive testing, tracking and other preventive measures, then the total net infected cases could peak in a month as the South Korean experience indicates. The net infected cases number refers to those currently testing positive for the coronavirus, minus those who have already recovered from the infection.
We have been analyzing data compiled by Johns Hopkins University’s Center for Systems Science and Engineering and have focused on two metrics. The first is the recovery rate, the percentage of patients who recover from COVID-19, the disease caused by the novel coronavirus, after a defined number of days. The second is the mortality rate, the percentage of patients who are confirmed to have COVID-19 and die after a defined number of days. If this description sounds confusing and you are mathematically inclined, then take a look at the two formulae below:
1) Recovery rate (“n” day lagged cases) = Cases recovered on a given date / Confirmed cases “n” days prior to that date
2) Mortality rate (“n” day lagged cases) = Deaths on a given date / Confirmed cases “n” days prior to that date
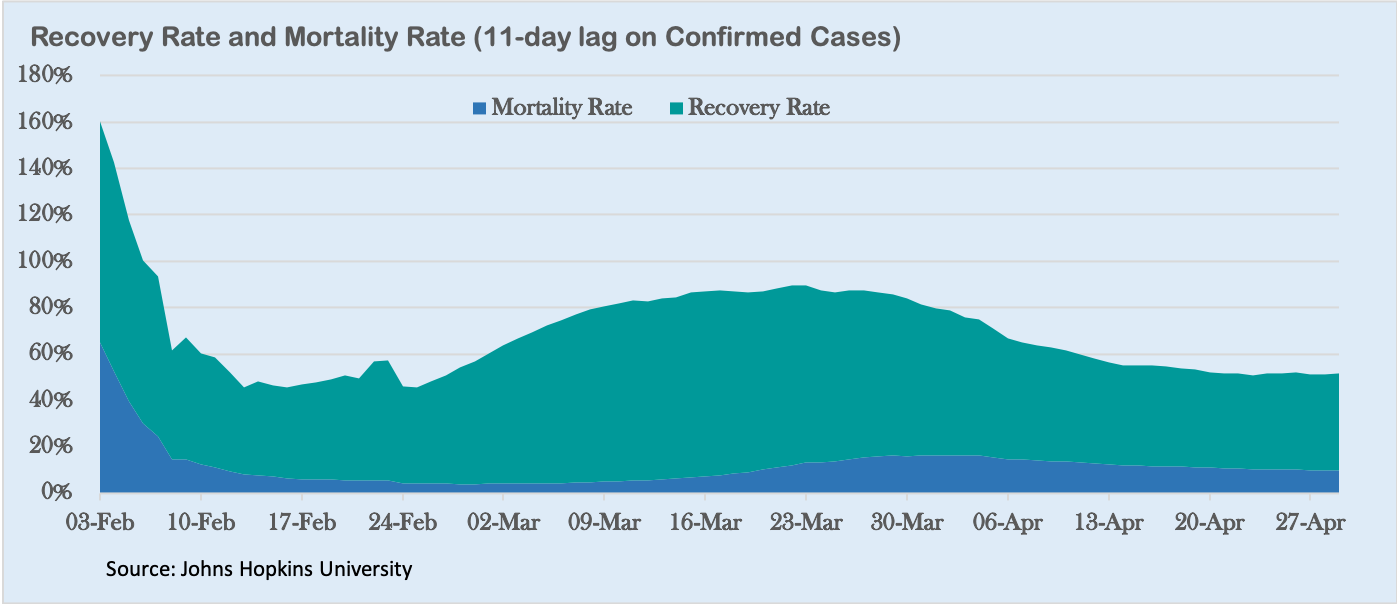
For confirmed cases, we found that the combined recovery rate and mortality rate to be under 100% after an 11-day time lag. For confirmed cases with a 15-day time lag, the combined recovery rate and mortality rate exceeds 100%, especially around late March and early April.
This does not make sense. It means more people were either recovering or dying than were infected 15 days ago. This tells us that case outcomes were achieved in less than 15 days around a month ago. People were recovering or dying within 15 days once medical professionals diagnosed them as confirmed cases. This has started to change in the latter half of April when the combined recovery and mortality rates are closer to 60%, implying longer periods to achieve outcomes. This is possibly due to more proactive testing worldwide.
Remember, most hospitals only test patients with visible COVID-19 symptoms. We know the period between infection and appearance of symptoms could be two weeks, especially for cases confirmed till mid-March. This tells us that those who can recover from COVID-19 do so within a month of infection.
Theoretically, if the US implemented policies like South Korea, COVID-19 could be checked in a month. However, the US is a federal nation with a strong culture of individualism and freedom. Different states have different policies. Even two cities within the same state might react differently. Until recently, college students were partying on Florida beaches during spring break. They have since gone back home to different parts of the country. Furthermore, domestic flights are still operating. This means a single infected person could infect many others on any flight.
It is unlikely that the US will be able to impose a draconian lockdown like China or even India. Therefore, we estimate that cases in the US would peak in about two months of lockdown, of which more than a month has already passed.
How Bad Could It Get?
In any infectious disease, the prevalence rate and mortality rate are the two key metrics to keep an eye on. The former is the ratio of confirmed cases to tested patients. We cannot calculate either of these metrics for the US with certainty because of a lack of data.
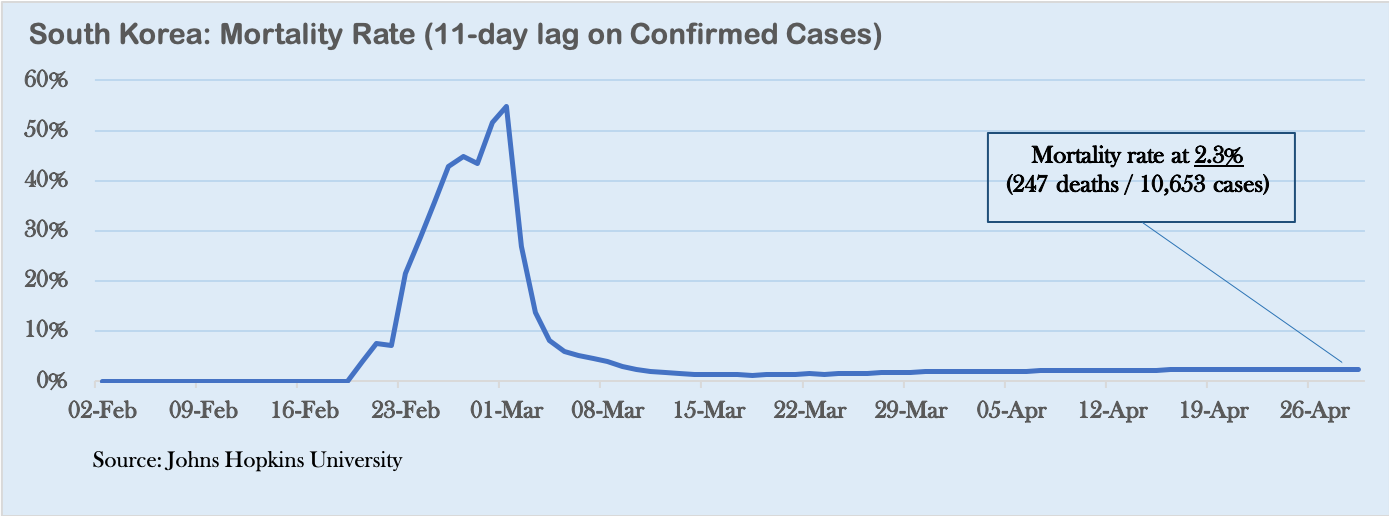
We can draw inferences from South Korea, though. South Korea followed a policy of aggressive testing for COVID-19. Its data tells us that the prevalence rate was approximately 3% and the mortality rate was 1.6%. In simple terms, this means that 3% of the “exposed” population contracted the disease and 1.6% of them died.
If the Korean prevalence rate holds true for the US and we assume the vast majority of about 320 million Americans to be exposed, we would have roughly 10 million cases in the country. If social distancing measures could contain the exposure to 10% to 20% of the American population, then the number of COVID-19 cases could be limited to up to 2 million.
Many governors and mayors across the US have acted resolutely. They have closed down offices and schools for the past few weeks. In New Jersey, New York, Connecticut and California, many of those who are observing social distancing are not displaying COVID-19 symptoms. Therefore, it might be fair to say that COVID-19 cases could potentially be limited to a few million in the US.
Medical reports indicate that between 2% to 6% of COVID-19 patients might need ventilators. This means the US might require up to 120,000 ventilators if we assume that 6% of 2 million patients would require them. The country already has 100,000 ventilators, but many of them are in use for patients in intensive care for other conditions. US President Donald Trump has promised to get 100,000 more ventilators in 100 days.
In theory, there should not be a shortage of ventilators, but distribution in a large country like the US is a challenge. There is a fair chance that hospitals in hotspots might run out of capacity, pushing up mortality rates. The American health care system would certainly be stretched, but it is unlikely to break down.
Is COVID-19 Seasonal?
As of now, we do not have enough evidence to conclude if COVID-19 is a one-off like the severe acute respiratory syndrome — known as SARS — or a recurring seasonal occurrence. We know that the novel coronavirus causing COVID-19 already has multiple strains. Viruses are known to mutate rapidly. That is why vaccines from one year often do not work during the next. COVID-19 could mutate and become more benign or more lethal. In the past, the Spanish Flu of 1918 became far more deadly in its subsequent two years.

There is reason to expect that the coronavirus could flare up again in late 2020 as things go back to normal and social distancing norms relax. However, it is reasonable to expect humanity to be better prepared to handle the pandemic. Health care capacity and systems are likely to improve. So will testing, contact tracing and traveler screening as well as containment, social and hygiene practices. Others are likely to learn from the experiences of Singapore, Taiwan and Hong Kong that have recorded significant success in curbing COVID-19.
Even if the virus comes back, we will be better prepared to face it. At this time of panic and even despair, we have reasons to be guardedly optimistic.
*[Sunil Asnani and Kshitij Bhatia are the founders and managing partners of First Principles Funds, an India-focused firm.]
The views expressed in this article are the author’s own and do not necessarily reflect Fair Observer’s editorial policy.
Support Fair Observer
We rely on your support for our independence, diversity and quality.
For more than 10 years, Fair Observer has been free, fair and independent. No billionaire owns us, no advertisers control us. We are a reader-supported nonprofit. Unlike many other publications, we keep our content free for readers regardless of where they live or whether they can afford to pay. We have no paywalls and no ads.
In the post-truth era of fake news, echo chambers and filter bubbles, we publish a plurality of perspectives from around the world. Anyone can publish with us, but everyone goes through a rigorous editorial process. So, you get fact-checked, well-reasoned content instead of noise.
We publish 3,000+ voices from 90+ countries. We also conduct education and training programs
on subjects ranging from digital media and journalism to writing and critical thinking. This
doesn’t come cheap. Servers, editors, trainers and web developers cost
money.
Please consider supporting us on a regular basis as a recurring donor or a
sustaining member.
Will you support FO’s journalism?
We rely on your support for our independence, diversity and quality.



















































The Hot Mic: Analyzing Biden’s 2nd Term, Chinese Spy Balloons, and Unstable Energy Markets
In a new series for FO° Podcasts—The Hot Mic—Atul Singh and Christopher Roper Schell examine US President Joe Biden’s State...




Commenting Guidelines
Please read our commenting guidelines before commenting.
1. Be Respectful: Please be polite to the author. Avoid hostility. The whole point of Fair Observer is openness to different perspectives from perspectives from around the world.
2. Comment Thoughtfully: Please be relevant and constructive. We do not allow personal attacks, disinformation or trolling. We will remove hate speech or incitement.
3. Contribute Usefully: Add something of value — a point of view, an argument, a personal experience or a relevant link if you are citing statistics and key facts.
Please agree to the guidelines before proceeding.